Expert Surgical Treatment by Dr. Rohit A. Thaker
Micro Endoscopic Minimally Invasive Spine Surgery in Ahmedabad
There is a step between traditional open spine surgery and full endoscopic spine surgery. It is called micro endoscopic minimally invasive spine surgery — sometimes shortened to MED, sometimes called tubular microscopic surgery. The technique uses a small tubular retractor about the diameter of a pencil, combined with a surgical microscope or an endoscope, to operate on the spine through a tiny incision while keeping the visualisation and instrumentation that a complex case sometimes demands. Dr. Rohit A. Thaker at Spine 360 offers Micro Endoscopic Minimally Invasive Spine Surgery in Ahmedabad as part of a complete minimally invasive spine practice — performed with the same fellowship-trained precision applied to all spine procedures here.

Understanding Micro Endoscopic Minimally Invasive Spine Surgery
The name itself is a bit confusing, so let’s be clear about what it actually means.
In micro endoscopic spine surgery, the operation is performed through a tubular retractor — a small rigid tube, usually around 16 to 22 millimetres in diameter — that is introduced through a small skin incision. Once the tube is in place, it pushes the back muscles aside without cutting them. The surgeon then operates inside the tube, using either an operating microscope for direct three-dimensional vision, or an endoscope attached to the tube for camera-based vision on a screen.

The key idea is that the spine is reached through a narrow corridor, not by exposing the entire surgical area. The muscles are dilated rather than dissected. Bleeding is minimal. Recovery is fast.
The technique sits between two well-known options. Traditional open surgery uses a 5 to 8 centimetre incision with the back muscles cut and pulled aside, giving the surgeon a wide direct view but doing significant tissue damage in the process. Full endoscopic surgery uses a 7 to 10 millimetre incision with a very narrow endoscope and works through tiny working channels, doing almost no tissue damage but with somewhat limited instrumentation. Micro endoscopic minimally invasive spine surgery sits in the middle — small incision, low tissue damage, but with more working space for complex problems.
The truth is that each technique has a sweet spot. The smartest practice is offering all of them and choosing the right one for each patient.
How Micro Endoscopic Minimally Invasive Spine Surgery Compares to Full Endoscopic Spine Surgery
This is the most important comparison for most patients reading this page, because the two techniques sound similar and they are often confused.
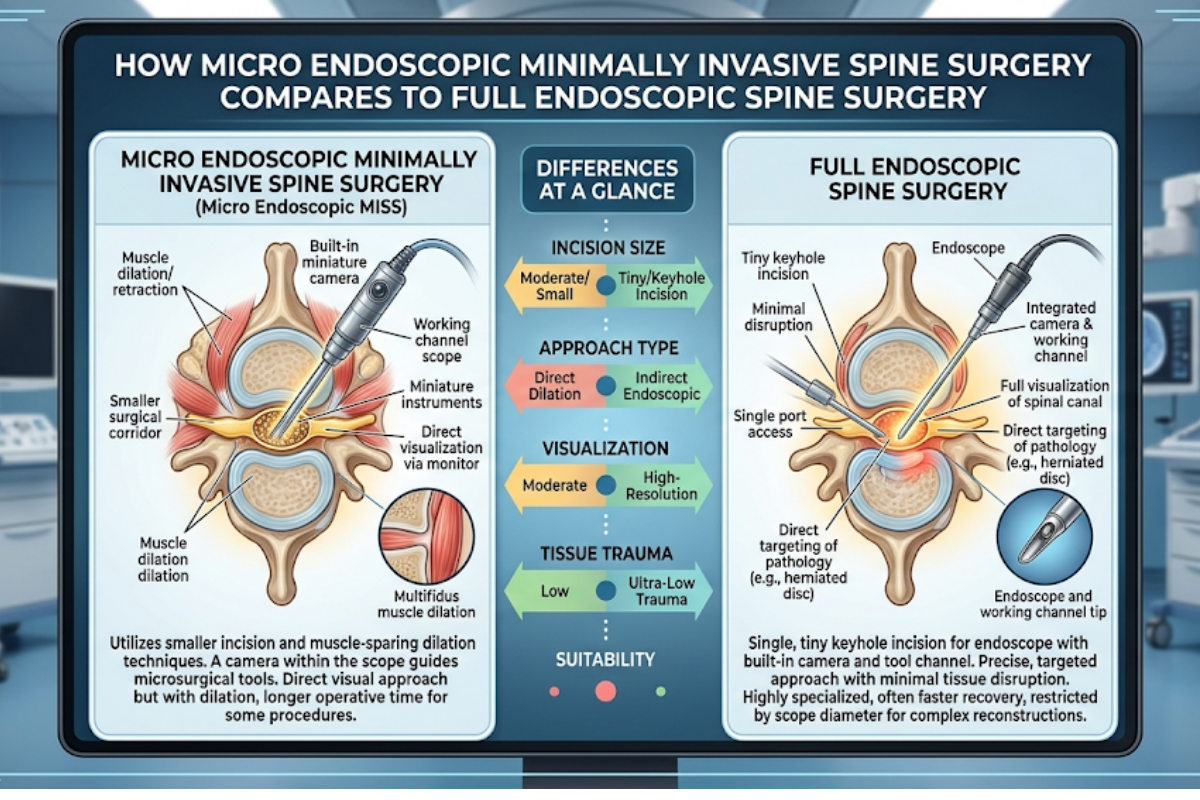
Neither technique is “better” in the abstract. They are different tools for different jobs. To be clear — when a case can be done either way with equal outcomes, full endoscopic offers slightly faster recovery. When the case is more complex, micro endoscopic gives the surgeon more room to work and is usually the right call.

FULL ENDOSCOPIC
- Incision: 7–10 mm
- Visualisation: 2D HD camera screen
- Instruments: Fine, narrow channels
- Best for: Clean disc herniations, selected stenosis
- Anaesthesia: Often local + sedation
- Office return: 2–3 weeks
MICRO ENDOSCOPIC
- Incision: 16–22 mm
- Visualisation: 3D surgical microscope
- Instruments: Standard spine tools
- Best for: Wider range — multi-level, revisions, fusion
- Anaesthesia: Usually general
- Office return: 3–5 weeks
The Role of the Surgical Microscope in Micro Endoscopic Spine Surgery
This is a specific feature worth understanding because it changes how surgery feels and how safely it is performed.
A surgical microscope is a large overhead device with high-magnification lenses, intense focused lighting, and binocular viewing. When the surgeon looks through it, the spinal anatomy is magnified ten to twenty times. The depth perception is true three-dimensional vision — no flat screen, no perspective compression. The surgeon sees the nerve, the disc, the bone, and the surrounding tissues in remarkable detail.
🔬 Why microscopic magnification means safer surgery
A 1 millimetre movement in the wrong direction can damage a nerve. Under microscopic magnification, what looks like 1 millimetre to the naked eye looks like 20 millimetres — and that visual room translates directly into safer surgery.
Combined with the tubular retractor, the microscope allows the surgeon to perform complex spine procedures through a small incision while maintaining the visual control that traditional open surgery offered. In many ways, this is the safest hybrid in modern spine surgery — small incision with full visual mastery of the surgical field.
For certain procedures — particularly microdiscectomy for disc herniations and microsurgical decompression for spinal stenosis — the microscope-based approach has been the global gold standard for decades. The micro endoscopic version simply makes the same procedure even less invasive.
Conditions Treated With Micro Endoscopic Minimally Invasive Spine Surgery
The technique is used across a broad range of spine problems — particularly those that need more than a simple disc removal but don’t quite need a full open surgery.
Lumbar disc herniation
microdiscectomy through a tubular retractor is one of the most performed procedures in modern spine surgery. Excellent for sciatica from a disc, with same-day or next-day discharge.
Lumbar spinal stenosis
microsurgical decompression is well-suited to widening the spinal canal in elderly patients and those with multi-level disease, where the tubular approach gives enough room for thorough decompression.
Cervical disc problems
posterior cervical foraminotomy through a tubular system is excellent for selected cervical radiculopathy, often avoiding the larger anterior cervical surgery.
Minimally invasive fusion (MIS TLIF, MIS PLIF)
The tubular approach allows placement of interbody cages and pedicle screws through small incisions, dramatically reducing blood loss and recovery time compared to open fusion.
Synovial cysts and facet joint cysts
these can be removed through a small tubular approach with minimal disturbance to the surrounding tissue.
Spinal tumor decompression in selected cases
minimally invasive approaches are increasingly used for spinal metastasis decompression in patients who cannot tolerate larger surgery.
Thoracic disc herniation
these are difficult cases to operate, and the tubular microsurgical approach is one of the safer ways to reach the thoracic disc without causing instability.
The point is that the micro endoscopic technique is not a niche option for one type of case. It is a workhorse method that covers a wide range of spine problems with significantly less trauma than open surgery.
What Actually Happens in the Operating Room
Patients are often curious about the actual sequence of events. Here is a realistic walkthrough.
Pre-Op
Pre-Operative Preparation
The patient meets the surgical and anaesthesia teams a day or two before. Blood work, ECG, anaesthesia assessment are completed. Blood thinners are stopped a few days in advance. An MRI of the relevant level is reviewed to plan the incision site and approach. The patient fasts for 6 hours before surgery.
Stage: 02
Incision and Tubular Retractor Placement
Under fluoroscopic guidance, the surgeon makes a small incision — usually about 18 to 22 millimetres long — at the precise level. A guide wire and then progressively larger dilators are introduced, gently spreading the back muscles apart. Once the correct depth is reached, the final tubular retractor — the working tube — is placed and locked in position.
Stage: 04
The Actual Procedure
Depending on what is needed — disc removal, ligament release, bone work for decompression, or screw and cage placement for fusion — the surgeon performs the procedure using standard or slightly modified spine instruments. The advantage of the tubular approach is that all of this is done in a controlled, narrow corridor with minimal blood loss and almost no collateral damage.
Stage: 01
On the Day of Surgery
The patient is admitted in the morning, IV access is set, vitals are monitored, and the patient is taken to the operating room. General anaesthesia is induced. The patient is positioned face down on a special operating table with a fluoroscopy unit positioned over the lumbar spine.
Stage: 03
Microscope or Endoscope in Position
The operating microscope is positioned above the tube, or the endoscope is attached. Either way, the surgeon now has a clear, magnified view down the tube to the spinal structures.
Stage: 05
Closure
The tubular retractor is removed. The muscles fall back into place naturally because they were never cut. The skin is closed with a few sutures or absorbable stitches. A small dressing is applied. The whole procedure typically takes 60 to 120 minutes depending on what is being done.
Immediate Recovery
The patient wakes up in recovery, is monitored for a couple of hours, and is then moved to the ward. Most patients are walking by evening of the same day or the next morning. Pain is usually well-controlled with simple oral painkillers because there is minimal wound trauma.
The Real Safety Advantage of Micro Endoscopic Spine Surgery
This is worth a section of its own because it gets discussed less than it should.
For most patients, these advantages are not just statistics. They are felt directly during recovery. The difference between recovering from an open lumbar surgery and a tubular minimally invasive surgery is significant enough that family members often comment on it.
Less tissue damage
Back muscles like the multifidus and erector spinae are preserved. Long-term spine stability, posture, and lower chronic pain follow.
Less blood loss
Most procedures lose under 50 ml — compared to 100–300 ml for an open equivalent. Matters especially for elderly and high-risk patients.
Lower infection risk
A smaller incision and a closed working corridor mean dramatically lower infection rates compared to open surgery.
Faster mobilisation
Patients walk earlier — reducing DVT, lung infection risk, and other immobility complications, particularly in the elderly.
Less post-operative pain
Less wound, less muscle trauma, less pain. Fewer painkillers, less opioid dependence, much better recovery experience.
Shorter hospital stay
Less exposure to hospital-acquired complications, faster return to a familiar home environment that supports faster healing.
Better long-term spinal mechanics
Preserving the spine’s natural structure means long-term outcomes — pain, function, recurrence — are at least as good as open surgery.
Visibly easier recovery
Family members often comment on the difference. The post-operative period feels nothing like what spine surgery used to mean.
Recovery After Micro Endoscopic Spine Surgery
The recovery is paced and predictable, with most patients hitting clear milestones.
The honest comparison is this — patients recovering from a micro endoscopic procedure usually do not need a week off bed rest, do not need round-the-clock home care, and do not need significant time in hospital. The whole experience is dramatically lighter than what spine surgery used to mean a decade ago.
Day 00
Day of Surgery
Patient wakes up in recovery, vitals are stabilised, and within a few hours is moved to the ward. Walking — assisted but on the patient's own legs — usually starts the same evening. Pain is mild to moderate, controlled with oral or IV painkillers.
DAY 01
Mobilisation
Most patients are mobilising independently. Walking up and down the corridor. Light meals, hydration, basic mobility exercises. Discharge is typically by evening of day 1 or morning of day 2.
WEEEk 01
Early Home Recovery
Walking 15 to 20 minutes, several times a day, at home. Some patients return to light desk work-from-home around day 5 to 7 if they feel up to it. Pain medication is mostly tapered. No bending, lifting, or twisting yet.
WEEEk 02 - 04
Return to Office Work
Most patients return to office work. Driving short distances becomes possible. Walking distance increases. Physiotherapy is started — gentle core activation, posture training, hip mobility work.
WEEEk 04 -08
Progressive Strengthening
Structured exercise progresses. Light gym activity, swimming, and stationary cycling are added. Walking is up to 30 to 45 minutes comfortably. Most patients describe themselves as "back to normal" by 6 to 8 weeks.
MONTH 3+
Full Activity Return
Heavier lifting, full gym training, and most sports are reintroduced in stages. Recovery is essentially complete by 3 months for the majority of patients.
The honest comparison is this — patients recovering from a micro endoscopic procedure usually do not need a week off bed rest, do not need round-the-clock home care, and do not need significant time in hospital. The whole experience is dramatically lighter than what spine surgery used to mean a decade ago.
Who Is and Isn't Suited For This Technique
Honest patient selection is what makes minimally invasive surgery work. The wrong patient operated through the wrong technique gives a poor outcome and a frustrated patient.
✓ Single-level or two-level lumbar disc herniation
✓ Lumbar spinal stenosis with multi-level involvement
✓ Recurrent disc problems with scar tissue from previous surgery
✓ Selected cervical radiculopathy from a lateral disc
✓ Patients needing instrumented fusion (MIS TLIF)
✓ Elderly or medically compromised patients who can’t tolerate open surgery
- Severe multi-level spinal deformity needing major correction
- Complex revision surgeries with extensive scarring at multiple levels
- Certain unstable spinal fractures needing wider exposure
• Tumor resections needing complete direct visualisation
For patients in the borderline zone, the choice often comes down to surgeon experience and judgment. Some experienced surgeons can perform complex cases through micro endoscopic techniques that would otherwise need open surgery. For straightforward cases, the technique is almost always the right call.
Why Patients Choose Dr. Rohit Thaker for Micro Endoscopic Spine Surgery
Surgical technique is only as good as the surgeon performing it. A few honest reasons patients choose this practice for minimally invasive spine surgery.
International fellowship training in minimally invasive spine surgery
Germany, Japan, and Israel are all global leaders in minimally invasive and tubular spine techniques. The fellowship exposure included high-volume training in both microsurgical and tubular endoscopic methods.
Full spectrum of techniques available
open surgery, microsurgical, micro endoscopic, full endoscopic, and image-guided pain procedures are all done under one roof. The patient gets the right technique, not the only one the surgeon knows.
Same-surgeon continuity
the same surgeon who consults you also operates and follows up. There is no fragmented care across multiple specialists.
Modern operating theatre
high-quality surgical microscope, fluoroscopy, neuromonitoring when needed, and all the supporting instrumentation required for safe minimally invasive surgery.
Honest case selection
minimally invasive surgery is offered when it genuinely helps and not when it doesn't. Open surgery is recommended without hesitation when that is the right answer for the patient.
Structured rehabilitation built in
post-operative recovery and rehabilitation are guided through structured protocols, ensuring that the gains of minimally invasive surgery translate into long-term outcomes.

Frequently Asked Questions
How is micro endoscopic surgery different from full endoscopic surgery?
Micro endoscopic uses a slightly larger tube (16-22 mm) and often a surgical microscope. Full endoscopic uses a 7-10 mm endoscope. Each suits different cases.
Will I need general anaesthesia for the surgery?
Yes, in most cases. A few procedures can be done under spinal or epidural anaesthesia. Local anaesthesia is rare for this technique.
How long is the hospital stay?
Usually 1 day. Most patients are discharged the evening of surgery or the next morning.
When can I return to office work?
Most patients return to desk work in 3 to 5 weeks. Heavier jobs need 6 to 8 weeks.
Will I have a visible scar?
The incision is small, usually 18 to 22 mm. The scar fades to a fine line within a few months.
Is this technique safe for elderly patients?
Yes, often safer than open surgery. Less blood loss, lower infection risk, and faster mobilisation make it especially suitable for older patients.
Can fusion surgery be done with this technique?
Yes. Minimally invasive fusion (MIS TLIF) places interbody cages and pedicle screws through small incisions with excellent results.
Does insurance cover micro endoscopic spine surgery?
Most major health insurance plans cover it. The clinic team helps with pre-authorisation and documentation.

Spine Specialist & Back Pain Expert
Clinic hours: Monday to Saturday | Emergency spine care available.