Expert Spine Treatment by Dr. Rohit A. Thaker
Spinal Fracture Treatment in Ahmedabad
A spinal fracture is one of those injuries where the next few hours genuinely matter. Whether it happened in a road accident, a fall from height, a sports injury, or even from a minor stumble in an elderly patient with osteoporosis — the spine has been damaged, and what gets done next can decide whether the patient walks normally again or lives with permanent disability. Dr. Rohit A. Thaker handles spinal trauma at Spine 360 in Ahmedabad, from simple compression fractures managed conservatively to complex unstable injuries needing emergency surgery. His fellowship training in Germany, Japan, and Israel included extensive exposure to spinal trauma — including high-velocity injuries, polytrauma cases, and pediatric spinal fractures.

Understanding Spinal Fracture — What Actually Breaks
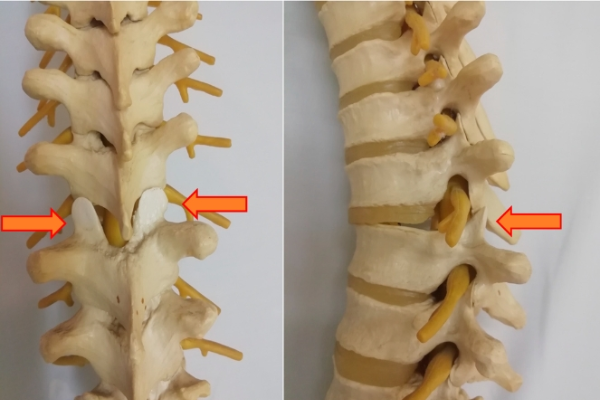
A spinal fracture means one or more of the bones in the spinal column — the vertebrae — has cracked, collapsed, or shifted out of place. The spine has 33 vertebrae arranged in a column, and any of them can be injured. But the most commonly fractured regions are the thoracolumbar junction (around T11 to L2) and the cervical spine (especially C1, C2, C5, C6, and C7).
A spinal fracture is not just about the bone. The real concern is what lies inside that bone — the spinal cord and nerve roots. If the fracture is stable and the cord is untouched, the patient may simply have pain and need rest and bracing. If the fracture is unstable, the broken pieces can press on or tear the spinal cord — and that is when paralysis becomes a real risk.
This is why every spinal fracture is graded on two parameters — how broken the bone is, and how much the neural elements are involved. The treatment is then decided around both.
Types of Spinal Fracture We Treat
Not every spinal fracture is the same. We see a wide range in clinic and casualty, and each one needs a slightly different approach.

Compression Fractures
The most common, especially in elderly patients with osteoporosis. The vertebral body collapses on itself, usually after a minor fall or even just lifting something heavy. The patient feels sudden, sharp back pain that worsens with movement. Most of these are stable and don’t damage the spinal cord.
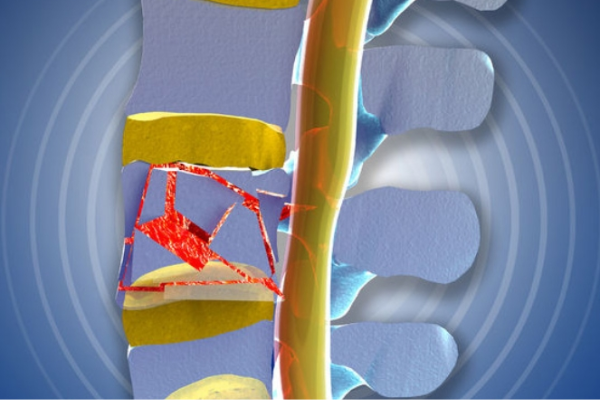
Burst Fractures
More serious. The vertebra shatters in multiple directions due to high-energy trauma falls from height, motor accidents and bone fragments can be pushed into the spinal canal. These often need surgery.
Fracture-Dislocations
The worst-case scenarios. The vertebrae are fractured *and* displaced out of alignment. The spinal cord is almost always involved. These are emergencies and need urgent stabilisation.
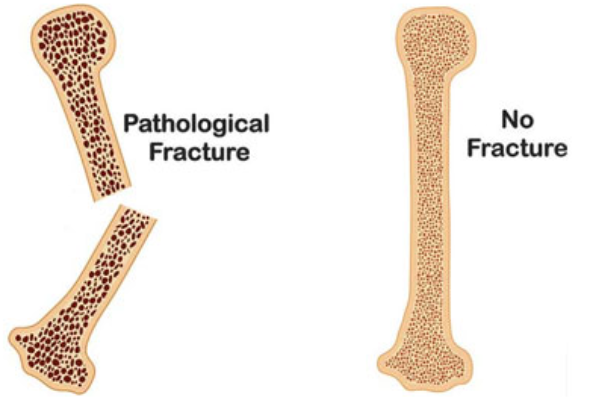
Pathological Fractures
Occur without significant trauma in patients whose vertebrae are already weakened by osteoporosis, spinal tumors, metastases, multiple myeloma, or infection. These need investigation for the underlying cause along with fracture management.
How Spinal Fracture Treatment in Ahmedabad Is Decided
Spinal fracture treatment in Ahmedabad at Spine 360 starts with one question — is the fracture stable, and is the spinal cord at risk? Everything else follows from there. Treatment falls into three broad pathways, and choosing the right one requires careful clinical judgment along with imaging.
1. Conservative (Non-Surgical) Management
The treatment includes a custom TLSO or cervical collar/Philadelphia collar brace for 6 to 12 weeks, pain medications, calcium and vitamin D supplementation, treatment of the underlying osteoporosis with bisphosphonates or teriparatide, gradual mobilisation, and structured physiotherapy.
2. Minimally Invasive Procedures
Vertebroplasty involves injecting bone cement into the fractured vertebra under image guidance to stabilise it. Kyphoplasty is a refinement of this where a small balloon is first inserted to restore vertebral height before cement is injected.
3. Surgical Stabilisation
Surgery is needed for unstable fractures, fractures with neurological deficit, dislocations, certain burst fractures, and traumatic deformities. The aim is to decompress the spinal cord, realign the spine, and stabilise it so healing can take place safely.
Symptoms and Red Flags After a Spine Injury
Some spinal fractures are obvious. Others are deceptively quiet. Here is what to actually look for.
The straightforward symptoms include severe back or neck pain after an injury, pain that gets worse with movement, muscle spasm, swelling or bruising over the spine, and difficulty standing or walking. Patients with pathological fractures often have no clear injury just sudden onset pain.

A common but dangerous mistake at accident sites is people trying to “help” by lifting or moving an injured person without spine support. If a spinal fracture is present and the spine is moved carelessly, a stable fracture can become unstable in seconds converting a recoverable injury into a paralysing one.

Get to a hospital immediately if any of these are present
Weakness or paralysis in the arms or legs, numbness or tingling below the level of injury, loss of bladder or bowel control, difficulty breathing after a chest or neck injury, a visible deformity in the back or neck, or loss of consciousness after the injury. Do not move the patient. Stabilise the head and neck, call for help, and let trained personnel transport with proper spinal precautions.
What to Do and What Not to Do — Quick Guide for Patients and Families
In a spinal injury, sometimes what you *don't* do matters as much as what you do.
✓ Keep the patient still
✓ Support the head and neck in a neutral position
✓ Call emergency services immediately
✓ Transport on a hard flat surface if absolutely necessary
✓ Inform the hospital in advance so a spine team is ready
✗ Make the patient sit up or stand to “check” if they are okay
✗ Twist or bend the neck
✗ Use a soft mattress or pillow under the injured area
✗ Give food or water in case surgery becomes urgent
✗ Delay imaging because “the pain isn’t that bad”
Why Patients Choose Dr. Rohit Thaker for Spinal Fracture Care
Spinal trauma is unforgiving. The decisions made in the first 24 to 72 hours often determine the long-term outcome — and that requires a surgeon who has handled enough cases to recognise patterns quickly.
Trauma-Trained at International Centres
Dr. Thaker's fellowships in Germany, Japan, and Israel included high-volume exposure to spinal trauma at centres receiving complex polytrauma cases regularly.
Comfortable Across the Full Range
From simple osteoporotic compression fractures needing a brace, to vertebroplasty and kyphoplasty, to complex unstable injuries requiring open or minimally invasive fixation. The decision is always based on what the patient actually needs, not what the surgeon prefers to do.
Minimally Invasive Trauma Surgery
Wherever possible, percutaneous and minimally invasive techniques are used to reduce blood loss, muscle damage, and recovery time. This matters particularly for elderly patients and polytrauma cases.
Coordinated Trauma Care
Spinal fractures rarely come alone. There are often head injuries, chest injuries, abdominal injuries, or limb fractures alongside. Working in coordination with neurosurgeons, orthopaedic trauma teams, and ICU specialists is part of how spine trauma is handled at Spine 360.
Long-Term Rehabilitation Planning
Fracture treatment doesn't end at the operating room. Physiotherapy, brace management, osteoporosis treatment, and gradual return to activity are guided over months, not weeks.

Frequently Asked Questions
Does every spinal fracture need surgery?
No. A large majority of spinal fractures — especially stable compression fractures and osteoporotic fractures — heal well with bracing, medication, and rest. Surgery is needed only for unstable fractures, neurological deficit, or specific high-risk patterns.
How long does a spinal fracture take to heal?
Most stable fractures heal in 6 to 12 weeks with bracing. Surgical cases typically need 3 to 6 months for full bone healing, though patients are usually walking and back to light activity much earlier.
Can I walk after a spinal fracture?
In most stable fractures, yes — usually with a brace and under guidance. In unstable fractures or fractures with cord injury, walking depends entirely on the type of injury and the recovery of neurological function. Early evaluation gives the best chance.
What is vertebroplasty and kyphoplasty?
These are minimally invasive procedures where bone cement is injected into a fractured vertebra to stabilise it and relieve pain. They are commonly used for osteoporotic compression fractures and pathological fractures. The procedure takes under an hour and most patients walk the same day.
Why do elderly people get spinal fractures so easily?
Osteoporosis weakens the bones with age, especially in women after menopause. The vertebrae become fragile and can fracture from even a small fall, a sneeze, or just lifting a heavy object. This is why bone health screening matters after the age of 50.
Is paralysis from a spinal fracture permanent?
It depends on the severity of cord injury. Some patients recover completely or partially with timely surgery and rehabilitation. Others may have lasting deficits. The earlier decompression and stabilisation are done, the better the chance of recovery.
What is the recovery time after spinal fracture surgery?
Most patients are mobilised within 1 to 2 days after surgery and discharged in 4 to 7 days. Light daily activities resume in 4 to 6 weeks. Full recovery, including return to work or sports, typically takes 3 to 6 months depending on the injury.
How can spinal fractures be prevented?
For elderly patients, this means treating osteoporosis with calcium, vitamin D, and bone-strengthening medications, doing weight-bearing exercises, fall-proofing the home, and wearing proper footwear. For younger people, it means seatbelt use, helmets for two-wheeler riders, and basic safety in sports and at work.

Spine Specialist & Back Pain Expert
Clinic hours: Monday to Saturday | Emergency spine care available.