Personalized Care for Lasting Result by Dr. Rohit A. Thaker
Lumbar Spondylosis Treatment in Ahmedabad
Most patients hear the word “spondylosis” and panic. The MRI report mentions “disc desiccation,” “osteophytes,” “facet hypertrophy,” and suddenly it sounds like the spine is falling apart. Honestly, in most cases, it isn’t. Lumbar spondylosis is essentially the wear and tear of the lower spine that happens to nearly everyone with age. The real question is not whether you have it, most adults above 40 do but whether it is actually causing your pain and what to do about it. Dr. Rohit A. Thaker at Spine 360 offers structured Lumbar Spondylosis Treatment in Ahmedabad built around finding the actual cause of pain, treating it properly, and avoiding the over-treatment that this condition commonly attracts.

Understanding Lumbar Spondylosis
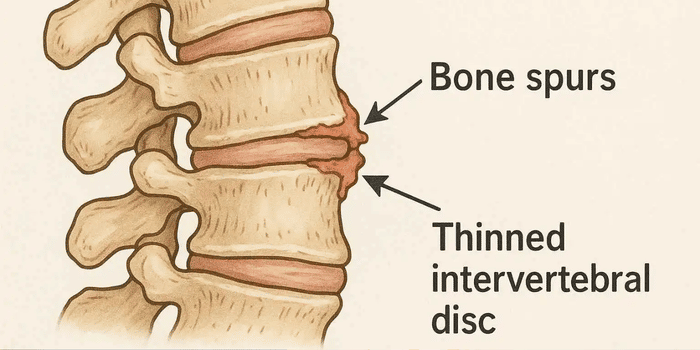
Lumbar spondylosis is the umbrella term for age-related degenerative changes in the lower spine. It is not a single disease. It is a slow process that involves the discs drying out, joints becoming arthritic, ligaments thickening, and small bony outgrowths called osteophytes developing along the vertebral edges.
The medical name comes from spondylos (vertebra) and -osis (a condition of). So spondylosis literally just means “a condition of the vertebrae,” usually degenerative. It is different from spondylitis (which is inflammatory and includes ankylosing spondylitis) and spondylolisthesis (where one vertebra slips forward over another). The three words sound similar and get confused often, even by doctors.
Most lumbar spondylosis affects the L4-L5 and L5-S1 levels, the lower two segments, because they take the most mechanical load. The C5-C6 region is the cervical equivalent.

A reassuring fact most patients are never told
Studies have shown that by age 60, around 90 percent of people have visible spondylotic changes on MRI and many of them have no pain whatsoever. That single fact changes how this condition should be treated. Think of it like grey hair or reading glasses. After a certain age, almost everyone shows some changes.
What Causes Lumbar Spondylosis — And What Doesn't
The honest list of causes is shorter than the internet makes it sound.

Age
the single biggest cause. Discs naturally lose water content as we get older. By 30, the disc is already drier than it was at 20. By 50, the changes are usually visible on imaging. This is normal biology, not a disease.

Lifestyle accelerators
long hours of sitting, poor posture, repetitive heavy lifting at work, and carrying weight badly. Smoking – yes, really. Obesity adds direct mechanical load on the lumbar spine over decades.
Genetics
disc degeneration runs in families. If your parents had bad backs in their fifties, your spine is more likely to follow the same pattern.

Old injuries
a bad fall in your twenties, a road accident, repeated minor strains at work can leave the spine slightly off-balance, and that asymmetry slowly grinds away one segment faster than the rest.
What doesn’t cause spondylosis: a single bad lift, sleeping in the wrong position, sitting on a particular chair, cracking your back. These can trigger acute episodes of pain in an already worn spine, but they don’t cause spondylosis itself.
This is worth saying directly. A lumbar spine MRI report on a 50-year-old almost always reads alarmingly. Words like “disc desiccation,” “annular tear,” “facet arthropathy,” “ligamentum flavum hypertrophy,” “foraminal narrowing,” “marginal osteophytes” all standard findings, most of them painless in most people. The MRI is a snapshot of structure. It does not tell us how much pain a patient is in. A patient with a clean MRI can be in agony, and a patient with a “terrible” MRI can have no symptoms at all. Both happen, often.
What matters is the match between the imaging findings and the patient’s actual symptoms. A herniated disc at L5-S1 is meaningful only if the leg pain matches that nerve root. Facet arthropathy is meaningful only if the back pain pattern fits. Osteophytes are meaningful only if they are actually compressing something.
Our job is to look at the patient first and the MRI second. Treating an MRI without listening to the patient is one of the most common reasons for unnecessary spine procedures.
Symptoms of Lumbar Spondylosis to Take Seriously
Many people with spondylosis on MRI have no symptoms at all. When symptoms do show up, they usually fall into a few clear patterns.
Chronic low back pain
A dull, deep ache in the lower back that comes and goes. Often worse in the morning, eases with movement, returns after sitting or standing too long.
Morning stiffness
Takes 15 to 30 minutes to loosen up. Different from inflammatory back pain (like ankylosing spondylitis) where stiffness lasts much longer.
Pain that radiates into the buttock or thigh
Usually when degenerative changes have started compressing a nerve root or when sacroiliac joints have become involved alongside.
Leg pain triggered by walking, relieved by sitting
Known as neurogenic claudication. This points to spinal stenosis, often a later stage of spondylosis. Patients say they can only walk for a few minutes before their legs feel heavy or numb.
Limited range of motion
Touching the toes becomes harder, getting up from a low chair takes effort.
Numbness, tingling, or weakness in the legs
Usually means a nerve root is involved and needs prompt evaluation.
Bladder or bowel problems with back pain
Rare but serious presentation that needs urgent attention. Cauda equina syndrome can develop in severe cases.
For most patients, the symptoms come and go in episodes, a few bad weeks, then months of relative quiet. The pattern of flare-ups, what triggers them, and what eases them, tells us more than any single MRI.
Lumbar Spondylosis Treatment in Ahmedabad — How We Actually Approach It
Lumbar spondylosis treatment in Ahmedabad at Spine 360 is built around one important truth: most patients improve with non-surgical care. Surgery has a real but limited role and it is reserved for specific situations where it will genuinely help. Treatment falls into clear stages, and most patients only need the early ones.
Stage: 01
Lifestyle and Basic Medical Care
This is the starting point. Pain medication for flare-ups (NSAIDs, muscle relaxants). Heat or ice. Activity modification, short-term reduction of aggravating activities. Weight management if overweight. Smoking cessation if relevant. Better posture, especially at work. Most acute episodes settle within 2 to 4 weeks.
Stage: 03
Image-Guided Pain Procedures
For pain that doesn't settle with medication and physio, targeted injections work very well. Facet joint injections for facetogenic pain. Medial branch blocks followed by radiofrequency ablation for chronic facet pain often gives 6 to 18 months of relief. Epidural steroid injections when there's nerve root involvement. Sacroiliac joint injections when the SI joint is part of the problem. All done under live fluoroscopy.
Stage: 02
Structured Physiotherapy
Probably the most underrated treatment for spondylosis. Targeted core strengthening, hip mobility work, hamstring stretching, lumbar stabilisation exercises. A good physio program changes the trajectory of spondylosis more than any pill ever will. We strongly recommend a structured 8 to 12 week program for almost every spondylosis patient.
Stage: 04
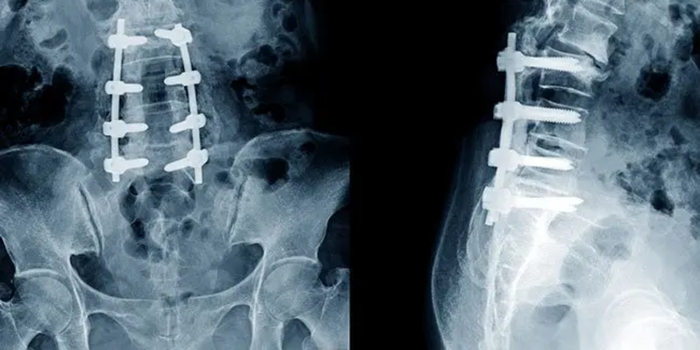
Surgery
Reserved for specific situations: significant spinal stenosis with walking limitation, instability (spondylolisthesis with symptoms), severe nerve compression with neurological deficit, or fractures and structural collapse. When surgery is needed, modern techniques are used endoscopic or minimally invasive decompression, microsurgical decompression, minimally invasive fusion where instability needs addressing. Most surgical patients walk within 24 hours and return to office work in 4 to 8 weeks.
The principle across all stages is the same: do the least that works. Move up only when necessary. Most spondylosis patients never reach stage four.
Beyond clinical treatment, this is honestly where most progress happens. Spondylosis is a long-term condition. What you do daily matters far more than what happens in clinic once a month.
✓ Walking 30 to 40 minutes most days
✓ Core exercises 3 to 4 times a week
✓ Stretching hips and hamstrings regularly
✓ Maintaining a healthy weight
✓ Medium-firm mattress with proper pillow support
✓ Standing breaks every 30 to 45 minutes
✓ Lifting with bent knees, weight close to body
✓ Quitting smoking
✗ Prolonged sitting and slouching
✗ Lifting with a curved back
✗ Sleeping on a sagging mattress
✗ Soft sofas for hours
✗ Carrying weight on one side
✗ Ignoring early warning twinges
✗ Smoking
✗ Sudden heavy weekend activity after sitting all week
Most patients who follow these habits consistently see their spondylosis become a much smaller problem over a year. Some find that their pain disappears almost entirely. It's not dramatic. It's just quietly consistent work.
When Lumbar Spondylosis Actually Needs Surgery
This question comes up in almost every consultation. Most spondylosis does not need surgery. The clear indications, the situations where surgery genuinely helps, are these:
For every other case — and that is the majority — surgery does not improve outcomes over good conservative care. We say so when that is true.
Over a period of three to six months following surgery, new bone grows through and around the graft material and interbody cage, eventually creating a solid bony bridge between the fused vertebrae. This process — called osseous fusion or arthrodesis — is confirmed by CT scan at follow-up.
Spondylolisthesis with Symptoms
When there is both back pain and nerve symptoms that have failed conservative care. Decompression with fusion in these cases gives long-term stability and pain relief.
Progressive Neurological Deficit
Increasing weakness, foot drop, hand clumsiness, or bladder/bowel issues. This shouldn’t be delayed.
Severe Life-Limiting Pain
When pain is severe despite all other treatments done properly for at least 3 to 6 months. This is a smaller group and decisions are made carefully.
Significant Spinal Stenosis with Neurogenic Claudication
When walking even 100 to 200 metres triggers leg heaviness, numbness, or pain. Decompression surgery in these cases is one of the most rewarding spine surgeries — patients walk further within weeks.
Instability from Fracture, Tumor, or Infection
These are different categories but can coexist with spondylosis and need surgical attention in their own right.
Why Patients Choose Dr. Rohit Thaker for Lumbar Spondylosis Treatment
There are many doctors treating spondylosis in Ahmedabad. The honest differences come down to a few things.
Honest assessment over MRI panic
Many patients arrive scared after reading their MRI report. The first consultation often involves explaining what the report actually means in their case — and that is sometimes the entire treatment some patients need.
Conservative care first, every time
Most spondylosis is managed without surgery. Medication, physiotherapy, lifestyle correction, and pain procedures handle the majority of cases successfully. Surgery is recommended only when it will genuinely change the outcome.
Image-guided pain procedures available in-house
Facet injections, radiofrequency ablation, epidural injections — all done at the same clinic under fluoroscopy. Patients don't need to bounce between specialists.
Modern surgical techniques when surgery is needed
Endoscopic decompression, minimally invasive fusion, microsurgical techniques — significantly reduced recovery time compared to traditional open surgery.
Long-term follow-up
Spondylosis is a long game. Patients are followed across years, not just one episode, so that small changes can be caught and addressed before they become big problems.

Frequently Asked Questions
Is lumbar spondylosis a serious condition?
Usually no. It is age-related wear and tear of the lower spine, and most people manage it well with medication, exercise, and lifestyle care.
Can lumbar spondylosis be cured?
The structural changes can’t be reversed, but the pain and stiffness can be controlled very well. Most patients live normal, active lives.
Does lumbar spondylosis always need surgery?
No. Around 85 to 90 percent of patients are managed without surgery. Surgery is only for specific cases like severe stenosis or instability.
What is the best exercise for lumbar spondylosis?
Walking, core strengthening, and hip and hamstring stretches are the most useful. Avoid heavy lifting and high-impact activities during flare-ups.
Is lumbar spondylosis the same as a slipped disc?
No. Spondylosis is general wear and tear. A slipped disc is one specific problem that can occur with or without spondylosis.
Will my MRI report mean I need surgery?
Not usually. MRI findings are common in middle-aged adults even without pain. Treatment is decided by symptoms, not by the MRI alone.
Can I prevent lumbar spondylosis from getting worse?
Yes. Regular exercise, healthy weight, good posture, no smoking, and avoiding heavy lifting all slow progression significantly.
When should I see a spine specialist for lumbar spondylosis?
If pain lasts more than 4 to 6 weeks, radiates to a leg, or comes with weakness, numbness, or bladder issues — see a specialist soon.

Spine Specialist & Back Pain Expert
Clinic hours: Monday to Saturday | Emergency spine care available.