Expert Spine Treatment by Dr. Rohit A. Thaker
Pain Procedure For Spine Conditions in Ahmedabad
There is a large group of patients who fall in an uncomfortable middle ground. Their back or neck pain hasn’t responded to painkillers and physiotherapy, but it isn’t quite bad enough to need surgery. They get told to “wait and watch” — and the pain just continues. For these patients, pain procedures often turn out to be the missing link. Dr. Rohit A. Thaker at Spine 360 offers a full range of image-guided spinal pain procedures in Ahmedabad — small, needle-based interventions done under live X-ray or ultrasound that target the exact source of pain. Most are done as day-care procedures, take less than an hour, and patients walk out the same day.

What Are Pain Procedure For Spine Conditions?
Spinal pain procedures are minimally invasive treatments designed to deliver medication, heat, or radiofrequency energy precisely to the structure causing the pain — whether it’s an inflamed nerve root, a worn-out facet joint, an irritated disc, or a damaged sacroiliac joint. They sit in the middle of the treatment ladder, between conservative care and open surgery.

The basic principle is simple. Spinal pain often comes from one specific structure — but pinpointing that structure is hard without precision tools. So under live imaging (fluoroscopy or ultrasound), a thin needle is guided to the exact spot, and the medication is delivered right where it is needed. This works far better than systemic painkillers, which flood the whole body and only partly reach the painful area.

Two roles, one procedure
These procedures are useful in two ways. Sometimes they are diagnostic — confirming which structure is actually generating the pain. Sometimes they are therapeutic — directly relieving the pain for weeks to months, often long enough for the underlying condition to heal on its own.
Common Pain Procedure For Spine Conditions We Perform
There isn’t one “spine injection” — there are several procedures, each targeting a different structure. Here is what we actually do in clinical practice.
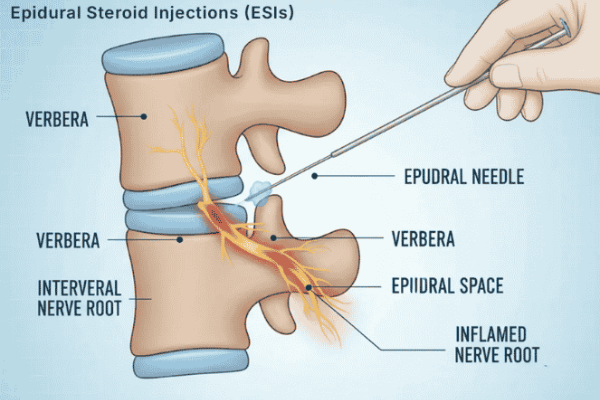
Epidural Steroid Injection
Probably the best known of the lot. A long-acting steroid mixed with local anaesthetic is delivered into the epidural space — the area just outside the dura covering the spinal cord. Used for radiating leg or arm pain from disc herniation, spinal stenosis, or post-surgical pain. Done in cervical, thoracic, or lumbar regions. Relief usually lasts weeks to months and can be repeated.
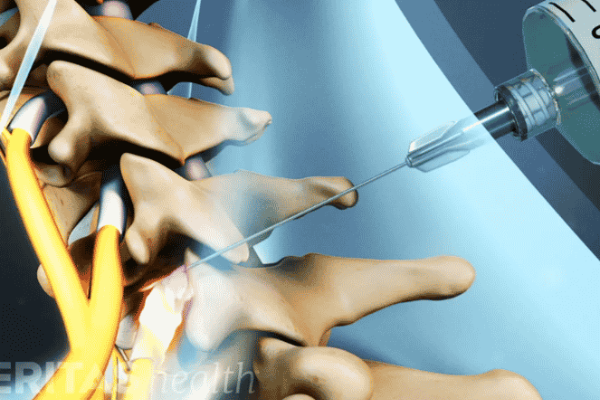
Transforaminal Nerve Root Block
A more targeted version of an epidural. The medication is delivered through the intervertebral foramen directly around the inflamed nerve root. Used mainly for sciatica or cervical radiculopathy when a specific nerve root is identifiable on MRI. Often gives better and faster relief than a regular epidural.
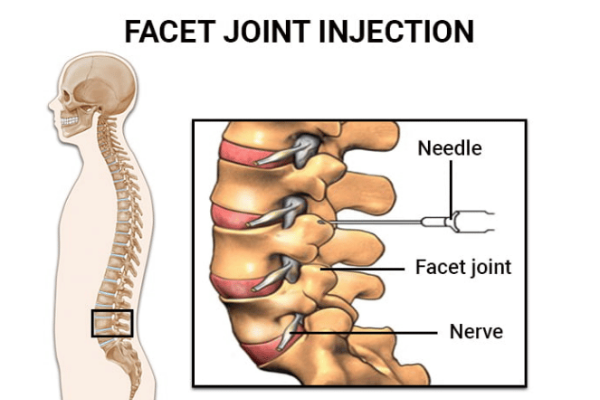
Facet Joint Injection
The facet joints are small paired joints at the back of the spine that can develop arthritis just like knee or hip joints. When they become painful, a small dose of steroid and local anaesthetic is injected directly into the joint under fluoroscopy. Very useful for chronic low back pain or neck pain that worsens with bending or twisting.
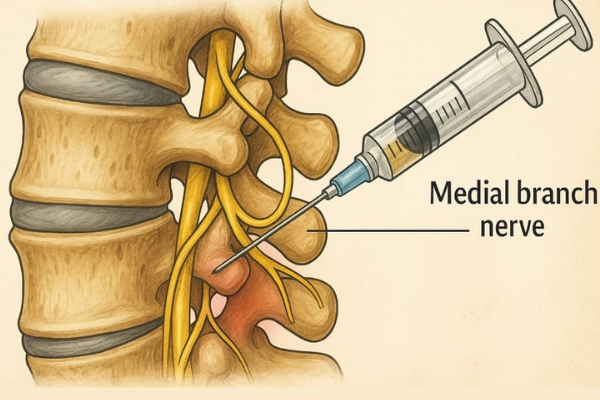
Medial Branch Block
This is a diagnostic-and-therapeutic test. The tiny nerve that supplies the facet joint is numbed with local anaesthetic. If the patient’s pain drops by more than 70 to 80 percent for the next few hours, the facet joint is confirmed as the pain source — and radiofrequency ablation can then be planned.
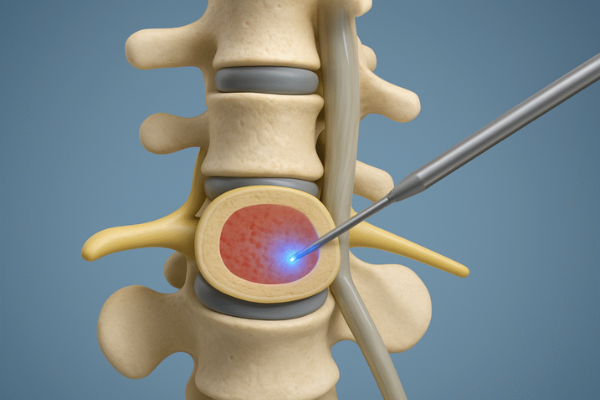
Radiofrequency Ablation (RFA)
One of the most underused but highly effective procedures. After a positive medial branch block, the same small nerves are heated using a radiofrequency probe under live imaging. This essentially “switches off” the pain signal from that joint for 6 to 18 months or longer. Excellent for chronic facetogenic back or neck pain.
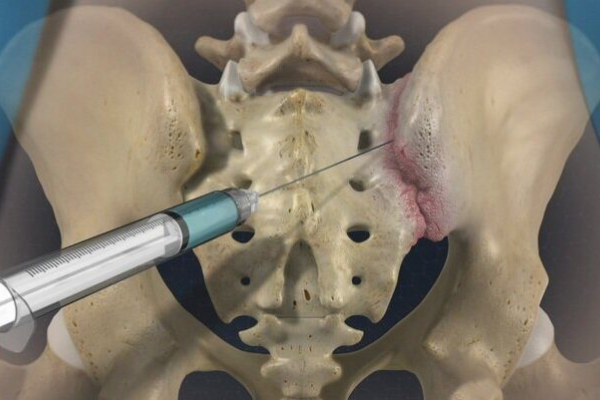
Sacroiliac Joint Injection
The SI joint is a common, frequently missed source of low back and buttock pain. Steroid and local anaesthetic are injected into the joint under fluoroscopy. Both diagnostic and therapeutic in nature.
Discography
A diagnostic test in which contrast dye is injected into a disc to identify if that particular disc is the source of pain. Used in selected cases before deciding on fusion or disc replacement.
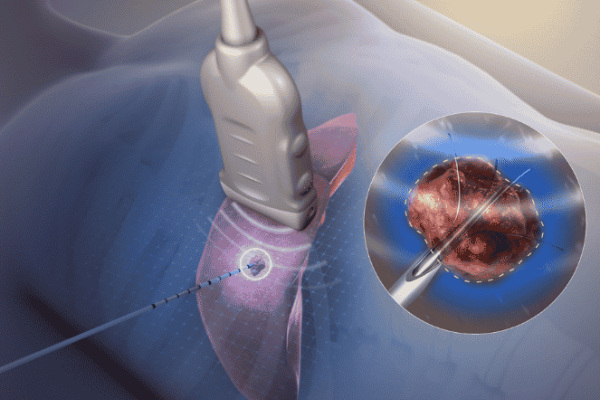
Nucleoplasty / Disc Decompression
For contained disc herniations, a small probe is introduced into the disc and a portion of the nucleus pulposus is ablated or removed. This reduces pressure on the nerve without open surgery. Done through a single needle puncture, no stitches.
How These Procedures Are Actually Done — Before, During, After
Patients often imagine these procedures to be more intimidating than they really are. Here is what actually happens.
Before the Procedure
A clinical evaluation is done to confirm that the pain pattern matches the planned procedure. Recent MRI or CT is reviewed. Blood thinners may need to be stopped a few days in advance. A short fasting period of 4 to 6 hours is advised. Diabetic patients are guided on sugar monitoring since steroids can transiently raise blood sugar.
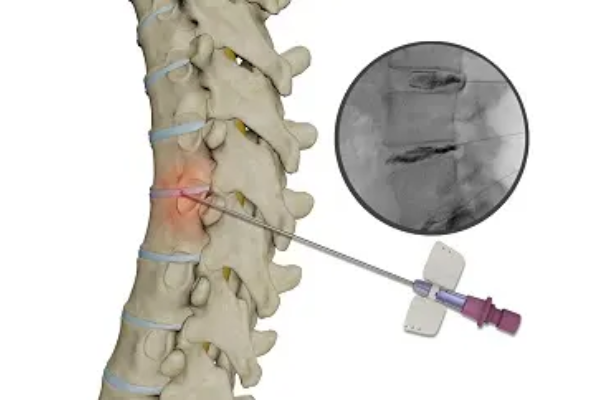
During the Procedure
The patient lies face down on a special table with a C-arm fluoroscopy unit above the spine. The skin is cleaned, draped, and numbed with local anaesthetic. The procedure needle is advanced under live imaging until it reaches the target. Contrast dye is sometimes injected first to confirm placement. Then the medication is delivered. Most procedures take 15 to 30 minutes.
After the Procedure
Patients rest for 30 to 60 minutes in a recovery area, walk around, and are discharged the same day. There may be mild soreness at the injection site for a day or two. Steroid effect starts in 3 to 7 days and reaches full effect by 2 weeks. Light activity resumes the next day; heavy lifting is avoided for a week.
Not every patient with back pain is a good candidate. The honest list of who actually benefits looks something like this.
Patients with acute disc-related sciatica where the pain is severe but the leg power is preserved — an epidural or transforaminal injection often relieves the pain enough for natural healing to take over. Patients with chronic facetogenic neck or back pain that worsens with bending, twisting, or extension — medial branch blocks followed by radiofrequency ablation can give months of relief. Elderly patients with lumbar spinal stenosis who can’t undergo major surgery — caudal or interlaminar epidurals offer meaningful symptom control. Patients with painful osteoporotic compression fractures — vertebroplasty or kyphoplasty often produces dramatic relief. Patients with post-surgical pain or scarring — caudal epidurals and adhesiolysis can be very useful. And patients with sacroiliac joint dysfunction — often misdiagnosed as disc disease — frequently respond beautifully to a single SI joint injection.
On the other hand, patients with severe progressive neurological deficits, large compressive disc fragments, or unstable spinal injuries are not good candidates. For those, surgery is the right answer, and pain procedures only delay the inevitable.
Why Patients Choose Dr. Rohit Thaker for Spinal Pain Procedures
Spinal pain procedures look simple on paper, but precision is everything. A few millimetres off-target and the procedure fails. Done well, the same procedure can transform a patient’s quality of life for months.
Performed Under Live Fluoroscopy or Ultrasound
Every procedure is done with real-time imaging. Blind injections, which are still done in some clinics, are unreliable and avoided here entirely.
Surgeon-Administered Procedures
Dr. Thaker performs these as a spine surgeon who also operates. That gives him a clearer sense of when a procedure will help and when surgery is actually the better option. Patients are not pushed toward injections endlessly when surgery is what they need.
Honest Expectations
Patients are told upfront what kind of relief to expect, how long it usually lasts, and what happens if the procedure doesn't work. No overpromising, no unrealistic claims.
Range of Options
From simple facet injections to radiofrequency ablation, nucleoplasty, and vertebroplasty, the full spectrum is available under one roof. Patients don't need to keep visiting different specialists.
Continuity of Care
If a procedure works, follow-up is planned. If it doesn't, the next step is discussed honestly. The relationship doesn't end at the injection table.

Frequently Asked Questions
Are spinal pain procedures painful?
Not usually. The skin is numbed with local anaesthetic first, and most patients describe only mild pressure or brief discomfort during the actual procedure. The entire process takes 15 to 30 minutes and is well-tolerated.
How long does the relief from a pain procedure last?
It varies. Epidural and transforaminal injections typically give relief for weeks to months. Radiofrequency ablation can give 6 to 18 months or more of relief. Repeat procedures are possible if needed.
Are these procedures a permanent cure?
For most cases, no — they manage the pain rather than cure the underlying condition. However, in acute disc herniations, the relief from an injection often gives the body enough time to heal naturally, and patients may not need anything further.
How many injections can be given in a year?
Most pain specialists limit epidural and joint injections to about 3 to 4 per year in the same area, mainly because of cumulative steroid exposure. Radiofrequency procedures and non-steroid options have different schedules.
Are there any side effects?
Common minor effects include local soreness, mild rise in blood sugar in diabetics, brief facial flushing, or temporary increase in pain for 1 to 2 days. Serious complications are very rare when procedures are performed under live imaging by experienced hands.
Can I avoid surgery with these procedures?
In many cases, yes — particularly for disc-related sciatica, facetogenic pain, and certain types of spinal stenosis. In other cases, pain procedures help temporarily but the underlying problem still needs surgery. An honest assessment makes all the difference.
Can diabetic and hypertensive patients undergo these procedures?
Yes, with proper precautions. Blood sugar may rise transiently with steroid injections, and diabetics are guided on monitoring. Blood pressure is checked before the procedure. These conditions are not absolute contraindications.
How soon can I resume normal activities after a procedure?
Most patients walk immediately after the procedure and resume routine activities the next day. Heavy lifting, gym workouts, and strenuous exercise are best avoided for about a week to allow the medication to work properly.

Spine Specialist & Back Pain Expert
Clinic hours: Monday to Saturday | Emergency spine care available.