Advanced Spine Care and Pain Relief
Minimally Invasive Spine Surgery in Ahmedabad
Spine surgery has undergone a significant transformation over the last two decades. What once required large incisions, extensive muscle stripping, prolonged hospital stays, and months of recovery can today be performed through incisions no larger than a centimetre, with patients walking the next morning and returning home within a day or two. This revolution in surgical technique is what defines minimally invasive spine surgery (MISS) — and it has fundamentally changed the outcome expectations for patients requiring surgical treatment of spinal conditions.
At Spine 360, Dr. Rohit Thaker — a spine surgeon with international fellowship training from Germany, Japan, and Israel — has been at the forefront of minimally invasive and endoscopic spine surgery in Ahmedabad. His clinical expertise spans the full spectrum of MISS techniques, from tubular micro endoscopic procedures to full endoscopic spine surgery, applied across a wide range of spinal conditions including disc prolapse, spinal stenosis, degenerative spondylosis, spinal instability, and deformity.

What is Minimally Invasive Spine Surgery?
Minimally invasive spine surgery refers to a collection of surgical techniques that access the spine through small incisions using specialised instruments, implants, and imaging guidance — rather than the large open incisions used in conventional spine surgery. The fundamental principle is to treat the targeted spinal pathology while causing the least possible disruption to the surrounding normal tissues — specifically the paraspinal muscles, ligaments, and bones that provide spinal stability.

The result is a procedure that achieves the same surgical goal, decompression of neural structures, stabilisation of unstable segments, or correction of deformity, while preserving the surrounding musculature, reducing blood loss, minimising postoperative pain, and shortening recovery time.

- Tubular retractor systems — Progressively dilating tubes that gently separate muscle fibres rather than cutting them, creating a working channel directly over the pathological spinal level
- Surgical endoscopes — High-definition cameras with integrated illumination that provide a magnified, detailed view of the operative field through a small working cannula, transmitted to a monitor in the operating room
- Fluoroscopy and intraoperative navigation — Real-time X-ray guidance and computer-assisted navigation systems that allow the surgeon to confirm instrument and implant positioning with precision throughout the procedure
- Percutaneous implant systems — Pedicle screws, interbody cages, and fixation rods that can be inserted through small stab incisions rather than large open exposures, used in minimally invasive spinal fusion procedures
Conditions treated through Minimally Invasive Spine Surgery
Conservative Management
Dr. Rohit Thaker performs minimally invasive surgical procedures for a wide range of spinal conditions at Spine 360. The choice of technique is guided by the specific diagnosis, the level and extent of spinal pathology, and the patient’s overall health and surgical fitness.
Lumbar Disc Prolapse (Slip Disc)
Herniation of the intervertebral disc causing compression of the exiting nerve root, resulting in sciatica and leg pain. Treated by endoscopic or tubular micro endoscopic discectomy, which removes the herniated disc fragment through a working cannula of less than 10 mm.
Cervical Disc Prolapse
Disc herniation in the neck region causing arm pain, numbness, or weakness. Managed by anterior cervical discectomy and fusion (ACDF) or posterior cervical foraminotomy using minimally invasive approaches.
Lumbar Spinal Stenosis
Narrowing of the spinal canal due to ligament thickening, facet joint overgrowth, and disc bulge causing neurogenic claudication and leg pain on walking. Treated by full endoscopic or tubular micro endoscopic decompression (laminotomy or foraminotomy).
Lumbar Spondylosis with Nerve Compression
Degenerative changes in the lower back with osteophytes and disc collapse compressing nerve roots. Addressed by endoscopic decompression with or without fusion depending on the presence of instability.
Degenerative Spondylolisthesis
Forward slippage of one vertebra over another due to disc and facet joint degeneration, causing spinal instability. Managed by minimally invasive transforaminal lumbar interbody fusion (MIS-TLIF) using percutaneous pedicle screws and interbody cages.
Spinal Fractures
Vertebral body fractures from trauma or osteoporosis treated by percutaneous pedicle screw fixation or balloon kyphoplasty, procedures performed through small stab incisions under fluoroscopic guidance.
Spinal Tumours
Primary and metastatic spine tumours requiring decompression and stabilisation are increasingly managed using minimally invasive approaches, reducing surgical morbidity in patients who are often already medically compromised.
Spinal Infections (TB Spine, Pyogenic Discitis)
Percutaneous drainage, biopsy, and stabilisation of infected spinal segments using minimally invasive fixation techniques.
Minimally Invasive Spine Surgery — Techniques Performed at Spine 360
Dr. Rohit Thaker is trained in the full range of minimally invasive spine surgery techniques, allowing him to select the most appropriate approach for each patient’s specific condition.

Full Endoscopic Spine Surgery
Full endoscopic spine surgery is the most minimally invasive surgical technique currently available for treating disc prolapse and spinal stenosis. The procedure uses a working cannula of approximately 7–10 mm in diameter, through which a high-definition endoscope is inserted. The surgeon visualises the entire operative field on a monitor and uses specialised instruments passed through the working channel to remove the compressive pathology, whether a herniated disc, thickened ligament, or osteophyte.
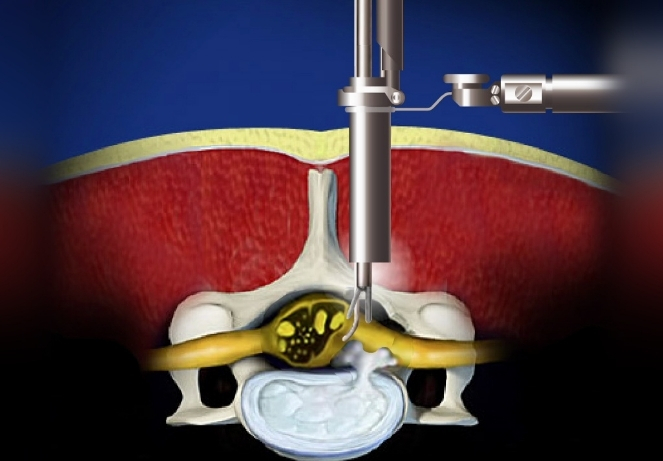
Micro Endoscopic Decompression / Discectomy (MED)
Micro endoscopic surgery uses a tubular retractor system of 16–18 mm that is introduced through sequential muscle dilation. An operating microscope or endoscope provides magnified visualisation, and conventional microsurgical instruments are used to perform the decompression. MED is particularly well-suited for cases requiring more extensive decompression at one or two spinal levels, or for surgeons transitioning from open microsurgery. Muscle damage is significantly reduced compared to open surgery, and recovery is considerably faster.
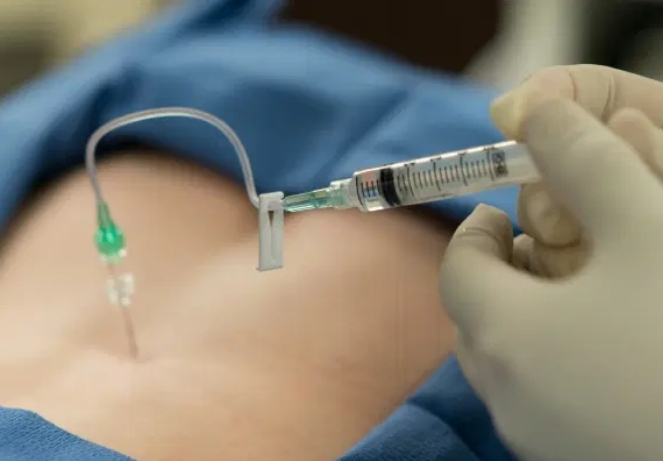
Image-Guided Spinal Injections
MIS-TLIF is the minimally invasive version of the conventional TLIF fusion procedure. It is performed for conditions such as degenerative spondylolisthesis, recurrent disc prolapse, lumbar instability, and multi-level degenerative spondylosis with collapse. Through two small bilateral incisions, percutaneous pedicle screws are inserted under fluoroscopic guidance, and an interbody cage is placed through a unilateral muscle-dilating tubular retractor. The fusion achieves decompression, disc height restoration, and segmental stabilisation without the large muscle dissection required in open fusion surgery.
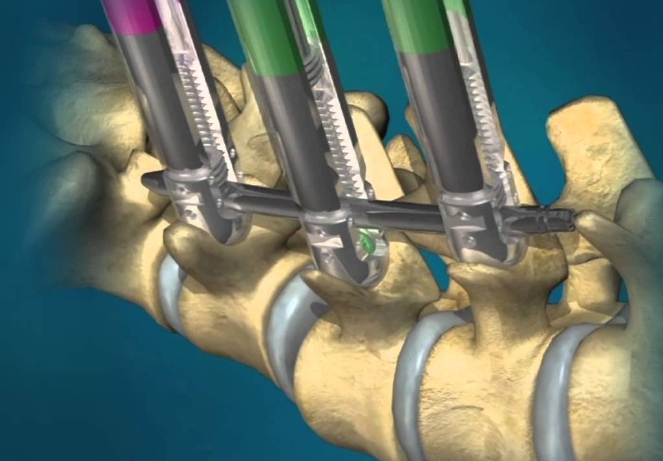
Percutaneous Pedicle Screw Fixation
In cases requiring multi-level spinal stabilisation, such as spinal fractures, tumour reconstruction, or long-segment deformity correction, percutaneous pedicle screws can be inserted through stab incisions under fluoroscopic or navigation guidance. The rods connecting the screws are passed in a subcutaneous tunnel, avoiding the need for open exposure of the entire spine.
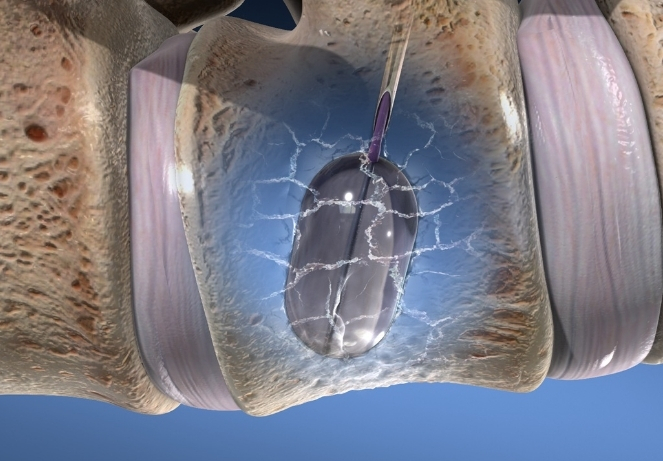
Balloon Kyphoplasty and Vertebroplasty
For osteoporotic vertebral compression fractures causing severe back pain, balloon kyphoplasty is a minimally invasive procedure in which a balloon is introduced into the collapsed vertebral body through a percutaneous needle, inflated to restore vertebral height, and the resulting cavity is filled with bone cement (PMMA). The procedure provides immediate pain relief, corrects vertebral deformity, and prevents further collapse.
Minimally Invasive Spine Surgery — Benefits Over Open Surgery
The clinical advantages of minimally invasive spine surgery over conventional open surgery are well-established in the international spine surgery literature and are consistently observed in Dr. Thaker’s practice at Spine 360.
- Significantly reduced postoperative pain — Minimal muscle disruption means far less tissue injury and consequently much lower levels of post-surgical pain. Most MISS patients require only oral analgesics rather than intravenous pain management.
- Minimal blood loss — Absence of large muscle dissection and the use of electrocautery-free endoscopic techniques result in negligible intraoperative blood loss, eliminating the need for blood transfusion in the vast majority of cases.
- Shorter hospital stay — Full endoscopic procedures are frequently performed as day-care or 23-hour admissions. Even fusion procedures using MIS techniques typically require only 2–3 days of hospitalisation.
- Faster return to daily activities — Most patients treated with endoscopic or tubular procedures return to light activities within 1–2 weeks and desk work within 3–4 weeks. Open surgery patients typically require 6–12 weeks before returning to comparable activity levels.
- Lower risk of surgical site infection — Smaller incisions with less exposed tissue significantly reduce the risk of wound complications and deep surgical site infections — particularly important in diabetic patients and the elderly.
- Preservation of spinal stability — By avoiding large-scale muscle and ligament stripping, MISS preserves the posterior tension band of the spine, maintaining spinal stability and reducing the risk of adjacent segment degeneration.
Why Choose Dr. Rohit Thaker for Minimally Invasive Spine Surgery in Ahmedabad
Choosing the right spine specialist makes a significant difference in long-term outcomes. Dr. Rohit Thaker combines academic depth, surgical skill, and an honest treatment philosophy.
Comprehensive MISS training
Fellowship training in Germany and Japan specifically covered advanced endoscopic spine surgery, percutaneous fixation, and MIS fusion techniques under internationally recognised faculty
Full spectrum of techniques available
From full endoscopic decompression at one end to MIS fusion and percutaneous fixation at the other, patients receive the technique most appropriate for their diagnosis — not the one available at a particular centre
Intraoperative navigation and fluoroscopy
Precision imaging is used throughout all MISS procedures to ensure accurate instrument and implant placement with safety
Honest surgical indication
MISS is not appropriate for every spine condition. Dr. Thaker’s practice emphasises selecting the right patients for surgery and the right technique for each patient, based on imaging findings and clinical severity

Frequently Asked Questions
Who is a suitable candidate for minimally invasive spine surgery?
Minimally invasive spine surgery (MISS) refers to surgical techniques that treat spinal conditions through very small incisions using specialised instruments, cameras, and real-time imaging guidance. Unlike open surgery, these techniques avoid cutting or stripping the muscles alongside the spine. The surgical outcome — decompression of nerves, stabilisation, or deformity correction — is the same as conventional surgery, but with less pain, less blood loss, and faster recovery.
Is minimally invasive spine surgery as effective as open spine surgery?
Yes. Multiple international studies and clinical trials have confirmed that minimally invasive spine surgery achieves equivalent neurological decompression and fusion rates compared to open surgery, with the added advantages of reduced blood loss, lower infection risk, shorter hospital stay, and faster functional recovery. For appropriately selected patients, MISS is now considered the preferred surgical approach.
Can sciatica be treated without surgery?
Procedure duration varies by the type of surgery and number of levels treated. A single-level full endoscopic discectomy or decompression typically takes 45 minutes to 1.5 hours. A minimally invasive fusion procedure (MIS-TLIF) at one level generally takes 2 to 3 hours. Multi-level procedures take proportionally longer. Dr. Thaker will discuss expected operative time during the pre-surgical consultation.
How long does minimally invasive spine surgery take?
Procedure duration varies by the type of surgery and number of levels treated. A single-level full endoscopic discectomy or decompression typically takes 45 minutes to 1.5 hours. A minimally invasive fusion procedure (MIS-TLIF) at one level generally takes 2 to 3 hours. Multi-level procedures take proportionally longer. Dr. Thaker will discuss expected operative time during the pre-surgical consultation.
How soon can I walk after minimally invasive spine surgery?
Most patients who undergo full endoscopic or tubular decompression procedures are able to walk the same day or the following morning. Fusion procedures require a slightly more gradual mobilisation, but patients are typically walking independently within 24 to 48 hours of surgery. Early mobilisation is actively encouraged as it reduces the risk of deep vein thrombosis and speeds up overall recovery.
Will I have a large scar after minimally invasive spine surgery?
No. Full endoscopic procedures leave incisions of less than 1 cm, and tubular micro endoscopic procedures typically require incisions of 1.5 to 2 cm. These small incisions heal well and leave minimal scarring. In contrast, open spine surgery typically requires incisions of 8 to 15 cm depending on the number of levels and type of procedure.
Is minimally invasive spine surgery available for the neck (cervical spine)?
Yes. Minimally invasive techniques are available for cervical spine conditions including disc prolapse, foraminal stenosis, and cervical myelopathy. Posterior cervical foraminotomy can be performed endoscopically or through a tubular retractor. Anterior cervical discectomy and fusion (ACDF) is itself a minimally invasive procedure by nature of the small anterior neck incision. Dr. Thaker assesses each cervical condition individually to recommend the appropriate approach.
Is the surgery performed under general anaesthesia?
Full endoscopic spine surgery can often be performed under local anaesthesia combined with intravenous sedation, which is a significant advantage for elderly patients or those with heart or lung conditions who carry higher risks under general anaesthesia. Tubular micro endoscopic procedures and fusion surgeries are generally performed under general or spinal anaesthesia. The anaesthetic plan is decided based on the procedure type and the patient’s medical condition after a pre-operative assessment.
If you have been advised spine surgery and want to explore whether a minimally invasive approach is possible for your condition, a consultation at Spine 360 will give you a clear picture of your options. Not every spine condition requires open surgery — and for those that can be treated with MISS, the difference in recovery experience is substantial.

Spine Specialist & Back Pain Expert
Clinic hours: Monday to Saturday | Emergency spine care available.