Advanced Spine Care and Pain Relief
Spinal Fusion Surgery in Ahmedabad
The human spine functions as a finely balanced mechanical structure each vertebral segment contributing to load bearing, movement, and the protection of the spinal cord and nerve roots. When one or more of these segments become structurally compromised through disc collapse, vertebral slippage, fracture, deformity, or infection the instability that results can cause chronic pain, nerve compression, and progressive deterioration of function. Spinal fusion surgery is the established surgical solution for restoring stability to these compromised segments, eliminating painful motion at the affected level, and creating the conditions for the spine to heal as a stable, well-aligned structure.
At Spine 360, Dr. Rohit Thaker a spine surgeon with international fellowship training from Germany, Japan, and Israel performs the full range of spinal fusion procedures, from single-level minimally invasive fusion to complex multi-level reconstructions. His surgical practice is built on precise preoperative planning, meticulous intraoperative technique, and a structured postoperative rehabilitation programme that ensures each patient achieves maximum functional recovery.

Spinal Fusion Surgery in Ahmedabad — What the Procedure Involves
Spinal fusion also referred to as spondylodesis or vertebral arthrodesis is a surgical procedure that joins two or more adjacent vertebrae into a single, solid bony unit. The fundamental goal is to eliminate the abnormal, painful movement at an unstable or degenerated spinal segment while maintaining or restoring correct spinal alignment.
Over a period of three to six months following surgery, new bone grows through and around the graft material and interbody cage, eventually creating a solid bony bridge between the fused vertebrae. This process called osseous fusion or arthrodesis is confirmed by CT scan at follow-up.

Bone graft
The biological material that promotes new bone growth between the vertebrae being fused. Bone graft can be harvested from the patient’s own iliac crest (autograft) considered the gold standard or sourced from a bone bank (allograft), or a combination of both.
Interbody cage
A structural implant typically made of PEEK (polyether ether ketone) or titanium that is placed within the intervertebral disc space after the disc is removed. The cage restores disc height, maintains foraminal height to decompress the nerve roots, and holds the bone graft.
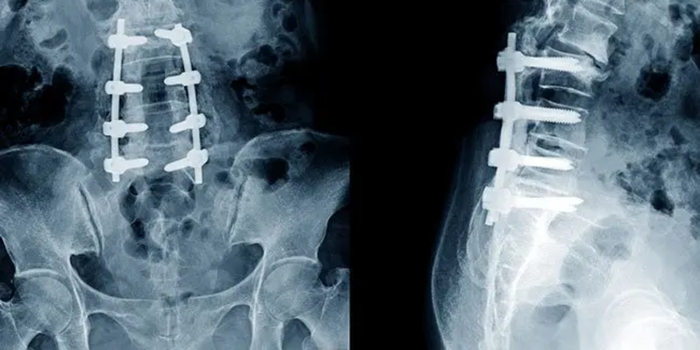
Pedicle screw-rod fixation
Titanium screws are inserted into the pedicles the strongest bony columns of the vertebra at each level being fused. The screws are connected by longitudinal rods, creating a rigid internal fixation construct that holds the fused segment in the correct position and alignment while the bone graft consolidates.
Conditions that Require Spinal Fusion Surgery
Spinal fusion is indicated when a spinal condition involves structural instability, significant deformity, or a level of degeneration that cannot be adequately addressed by decompression alone. The following conditions are the most common indications for spinal fusion surgery at Spine 360.
Degenerative spondylolisthesis is the forward slippage of one vertebral body over the one below it, caused by facet joint and disc degeneration at the affected level. It most commonly occurs at the L4-L5 level. The resulting spinal instability and canal narrowing cause back pain, neurogenic claudication, and radicular leg pain. Decompression alone in this setting is insufficient as removing the posterior elements without stabilisation worsens the listhesis. Fusion with decompression corrects the slippage, stabilises the segment, and relieves the neural compression.
Severe intervertebral disc degeneration with significant disc height collapse, end-plate changes, and segmental instability on dynamic X-rays causes chronic mechanical back pain and reduced functional capacity. When conservative treatment fails over an adequate period, fusion of the affected level with an interbody cage eliminates the painful disc motion, restores disc height, and decompresses the associated foraminal narrowing.
Unstable fractures of the thoracic or lumbar spine — particularly burst fractures with canal compromise and fracture-dislocations — require surgical stabilisation to protect the spinal cord and nerve roots, restore vertebral alignment, and allow early mobilisation. Posterior pedicle screw fixation with or without interbody cage placement achieves immediate stability while the fracture heals.
Primary and metastatic spinal tumours that compromise vertebral structural integrity require surgical resection and spinal reconstruction to prevent pathological fracture and neurological deterioration. Spinal fusion with long-segment pedicle screw fixation and anterior cage reconstruction restores stability after tumour resection.
Isthmic spondylolisthesis results from a defect or stress fracture in the pars interarticular is the narrow bridge of bone connecting the superior and inferior facets of a vertebra. This allows the vertebral body to slip forward, stretching and compressing the exiting nerve roots. It most commonly affects the L5-S1 level and frequently presents in younger patients. Spinal fusion restores stability at the defect level and decompresses the affected nerve roots.
In patients with spinal stenosis where the compressive changes are associated with underlying segmental instability or spondylolisthesis, decompression alone risks further destabilising the affected level. In these cases, decompression is combined with instrumented fusion to ensure long-term stability and prevent recurrence of symptoms due to progressive listhesis.
Adult degenerative scoliosis a lateral curvature of the spine developing in adulthood due to asymmetric disc and facet joint degeneration and kyphotic deformity from osteoporotic fractures or ankylosing spondylitis can cause progressive pain, postural imbalance, and nerve compression. Multi-level fusion with deformity correction realigns the spine in the sagittal and coronal planes, relieves neural compression, and prevents further curve progression.
Infections of the intervertebral disc and adjacent vertebral bodies including tuberculosis (Pott’s disease) and pyogenic bacterial discitis cause vertebral destruction, kyphotic deformity, and spinal cord or nerve root compression. Surgical débridement of the infected tissue combined with anterior column reconstruction using a titanium cage and posterior instrumented fusion restores spinal stability and corrects the infectious kyphosis.
Spinal Fusion Surgery — Types of Fusion Procedures Performed at Spine 360
The choice of fusion technique depends on the diagnosis, the spinal level, the degree of instability, the surgical approach best suited to the pathology, and patient-specific factors. Dr. Rohit Thaker is trained in all major spinal fusion approaches and selects the most appropriate technique for each case.
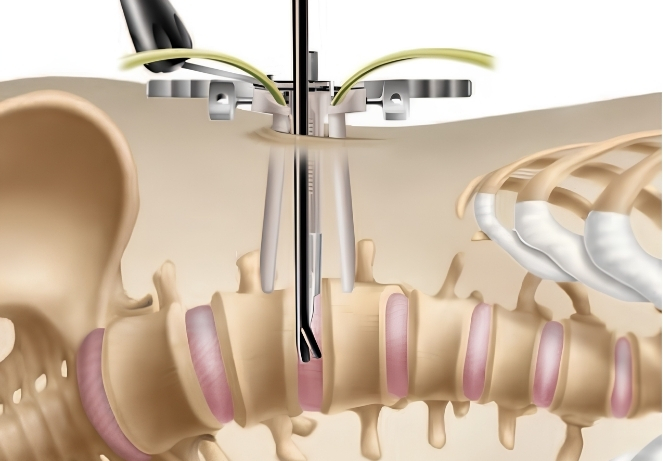
Transforaminal Lumbar Interbody Fusion (TLIF)
TLIF is performed through a posterior midline or paramedian incision. Access to the disc space is obtained through the neural foramen after partial removal of the facet joint on one side. The disc is removed, an interbody cage packed with bone graft is inserted, and bilateral pedicle screws and rods complete the fixation construct. TLIF is versatile, avoids the risks of anterior abdominal approach surgery, and can be performed in a minimally invasive version (MIS-TLIF) through two small incisions using percutaneous screws and a tubular retractor for cage insertion.

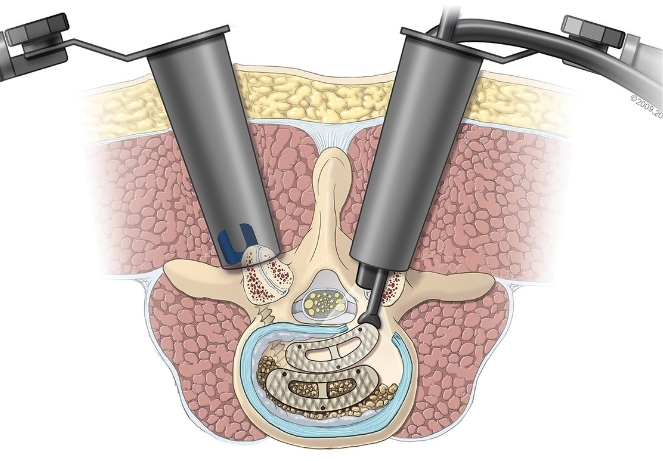
Posterior Lumbar Interbody Fusion (PLIF)
PLIF accesses the disc space directly through the posterior midline after retraction of both nerve roots. Two smaller interbody cages are placed bilaterally within the disc space, combined with pedicle screw-rod fixation. PLIF provides bilateral cage support and direct visualisation of the nerve roots during decompression but requires more neural retraction than TLIF. It is particularly suited for cases with significant bilateral disc and foraminal pathology.
Anterior Lumbar Interbody Fusion (ALIF)
ALIF approaches the lumbar disc space directly through the anterior abdomen, avoiding the posterior spinal muscles entirely. A large footprint interbody cage — covering the maximum surface area of the vertebral endplates — provides excellent disc height restoration and sagittal balance correction. ALIF is particularly effective for L4-L5 and L5-S1 pathology and is frequently combined with posterior fixation in a combined anterior-posterior fusion for multi-level deformity correction.
Extreme Lateral Interbody Fusion (XLIF / LLIF)
XLIF accesses the lumbar disc space through the patient’s flank — between the ribs and the iliac crest — using a lateral retroperitoneal approach through the psoas muscle with neurophysiological monitoring. A wide interbody cage is placed across the full width of the disc space, providing excellent coronal and sagittal plane correction. XLIF is particularly valuable in adult degenerative scoliosis correction and multi-level disc degeneration requiring minimal surgical morbidity, as it avoids both the posterior musculature and the anterior abdominal vessels.
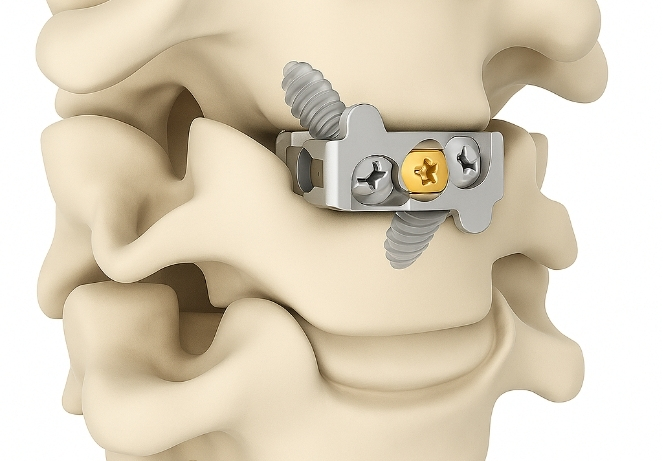
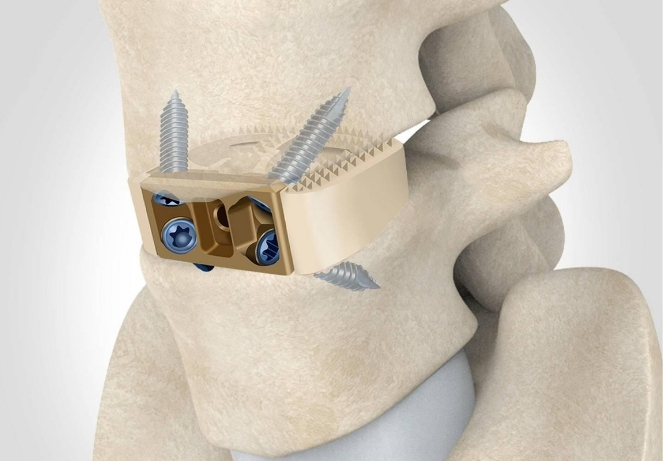
Anterior Cervical Discectomy and Fusion (ACDF)
For cervical disc prolapse and cervical spondylotic myelopathy requiring surgical treatment, ACDF is the standard procedure. Through a small anterior neck incision, the degenerated disc and any compressive osteophytes are removed, a cage packed with bone graft is placed in the disc space, and a titanium plate with screws secures the fusion construct. ACDF reliably decompresses the spinal cord and nerve roots and achieves solid fusion in the vast majority of cases.
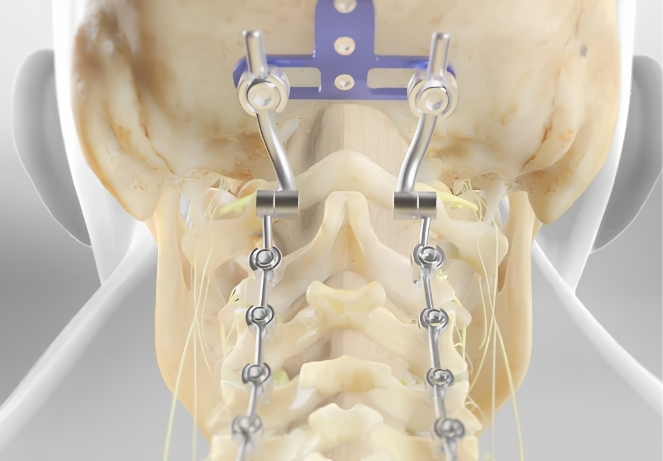
Posterior Cervical Fusion and Occipitocervical Fusion
When cervical instability spans multiple levels, involves the craniocervical junction, or results from trauma, rheumatoid arthritis, or congenital anomalies, posterior cervical or occipitocervical fusion using lateral mass screws, pedicle screws, and rod fixation restores stability to the upper and mid-cervical spine.
Spinal Fusion Surgery — What to Expect Before and After Surgery
Prior to spinal fusion surgery, a comprehensive preoperative assessment is conducted including MRI, CT scan with 3D reconstruction for surgical planning, dynamic X-rays to assess instability, baseline blood investigations, cardiac and anaesthetic fitness evaluation, and — in cases requiring bone graft — a DEXA scan to assess bone density. Patients on blood thinners, anti-inflammatory medications, or biologic agents are given specific instructions on when to stop these prior to surgery. Preoperative physiotherapy may be recommended to optimise core muscle strength before the procedure.
Spinal fusion surgery is performed under general anaesthesia. Hospital stay ranges from 3 to 5 days depending on the complexity of the procedure and the number of levels fused. Patients are mobilised with physiotherapy support on the first or second postoperative day. A lumbar brace may be recommended for 6 to 12 weeks in selected cases to provide external support during the early fusion phase. Drain tubes, if placed, are removed within 24 to 48 hours.
The internal fixation provided by the pedicle screws and rods holds the spine stable immediately after surgery. Bone fusion — the biological process of new bone bridging the fused segment — takes 3 to 6 months to achieve solid consolidation, confirmed by CT scan at the follow-up visit. Full return to non-physical work typically occurs in 6 to 8 weeks. Return to physical labour, sport, or strenuous activity is assessed individually, generally at 3 to 6 months following surgery.
Why Choose Dr. Rohit Thaker for Spinal Fusion Surgery in Ahmedabad
Choosing the right spine specialist makes a significant difference in long-term outcomes. Dr. Rohit Thaker combines academic depth, surgical skill, and an honest treatment philosophy.
Rigorous surgical indication
Fusion is a significant procedure with a defined recovery period. It is recommended only when there is a clear structural basis for instability, confirmed on imaging and correlated with clinical symptoms. Conservative treatment is fully exhausted before fusion is considered except in emergencies.
Minimally invasive fusion first
Where the diagnosis and anatomy allow, MIS-TLIF and percutaneous fixation are offered in preference to open fusion, reducing muscle damage, blood loss, and recovery time while achieving equivalent fusion rates.
Advanced implant systems
Titanium pedicle screws, PEEK and titanium interbody cages, and bone graft substitutes used at Spine 360 meet international quality and biocompatibility standards.
Intraoperative navigation and neuromonitoring
Computer-assisted navigation and intraoperative neurophysiological monitoring (IONM) are used in complex fusion cases to ensure precise implant placement and continuous monitoring of spinal cord and nerve root function throughout the procedure.

Frequently Asked Questions
What is spinal fusion surgery?
Spinal fusion surgery is a procedure that permanently joins two or more vertebrae together using bone graft, an interbody cage, and metal screws and rods. The goal is to eliminate painful or abnormal movement at an unstable spinal segment, correct deformity, or stabilise the spine after fracture, infection, or tumour. Over several months after surgery, new bone grows between the fused vertebrae, creating a solid, stable unit.
How do I know if I need spinal fusion or just a decompression?
Decompression surgery alone is appropriate when the primary problem is nerve compression without significant spinal instability — such as a simple disc prolapse or spinal stenosis in a stable spine. Fusion is required when there is slippage of one vertebra over another (spondylolisthesis), significant disc collapse causing instability, spinal fracture, deformity, or when prior decompression has destabilised the spine. Dr. Thaker determines the appropriate procedure based on clinical examination, MRI, and dynamic X-rays.
Will spinal fusion restrict my movement permanently?
A single-level spinal fusion has a minimal effect on overall spinal mobility in most patients. The lumbar spine has multiple segments, and adjacent levels compensate for the fused level without producing noticeable restriction in daily activities. Multi-level fusion across several vertebrae does reduce overall spinal movement to a greater extent, but the functional improvement achieved by eliminating the pain and instability typically outweighs the reduction in movement. Physiotherapy after surgery helps restore the maximum possible functional range.
Is spinal fusion a major surgery? What are the risks?
Spinal fusion is a significant surgical procedure, and the risks vary depending on the approach, number of levels fused, and the patient’s overall health. Potential risks include infection, blood loss, nerve root injury, dural tear (cerebrospinal fluid leak), implant-related complications, non-union (failure of bone fusion), and adjacent segment degeneration over time. In experienced hands with modern techniques and implants, the rates of serious complications are low. Dr. Thaker discusses all relevant risks in detail during the preoperative consultation.
How long does it take for spinal fusion to fully heal?
The internal fixation provided by the pedicle screws and rods stabilises the spine immediately after surgery. Solid bone fusion — the biological process of new bone bridging the fused segment — takes 3 to 6 months. Full bone consolidation is confirmed by CT scan at the follow-up review. The metal implants remain permanently and provide long-term stability regardless of the fusion status.
What is the difference between TLIF and PLIF?
Both TLIF and PLIF are posterior lumbar interbody fusion techniques that place a cage in the disc space from a posterior approach. The difference lies in how the disc space is accessed. TLIF enters the disc space through the neural foramen on one side after partial facet removal, requiring less nerve root retraction and using a single larger cage. PLIF accesses the disc space directly from behind after retracting both nerve roots bilaterally, using two smaller cages. TLIF is the more commonly performed technique today due to its lower risk of nerve root injury and equivalent fusion outcomes.
Can spinal fusion be done using minimally invasive techniques?
Yes. Minimally invasive spinal fusion — specifically MIS-TLIF — is now well-established and is the preferred approach for single and two-level lumbar fusion in appropriate patients. Through two small posterior incisions, percutaneous pedicle screws are inserted under fluoroscopic guidance, and the interbody cage is placed through a tubular retractor. Blood loss, muscle damage, and recovery time are significantly reduced compared to open fusion, with equivalent fusion rates and clinical outcomes.
What happens if spinal fusion fails or does not heal properly?
In a small percentage of cases, the bone graft does not consolidate into a solid fusion — a condition called pseudarthrosis or non-union. This may cause persistent or recurrent back pain, implant loosening, or screw breakage. Risk factors include smoking, osteoporosis, obesity, diabetes, and multi-level fusion. If pseudarthrosis is confirmed on CT scan, revision surgery with additional bone graft, improved fixation, or biological enhancement agents may be required. Following postoperative instructions, attending regular follow-ups, and avoiding smoking are the most important factors in achieving successful fusion.

Spine Specialist & Back Pain Expert
Clinic hours: Monday to Saturday | Emergency spine care available.